Background: The SAMHSA/Ce-PIM partnership was formed nearly five years ago between the Substance Abuse and Mental Health Service Administration and the Center for Prevention Implementation Methodology (Ce-PIM) for Substance Abuse and HIV, which is funded by NIDA. We discuss principles behind this partnership model that links service delivery at a national level and research to prevent of substance misuse, mental disorders and suicide, and HIV Transmission.
Approach: The formation of this partnership was guided by Sheppard Kellam’s model of partnership building. We use cultural exchange theory, to monitor how this partnership evolves over stages, identifying key milestones and assessing both process and outcomes. Further, we discuss this partnership from both SAMHSA’s and Ce-PIM’s perspectives.
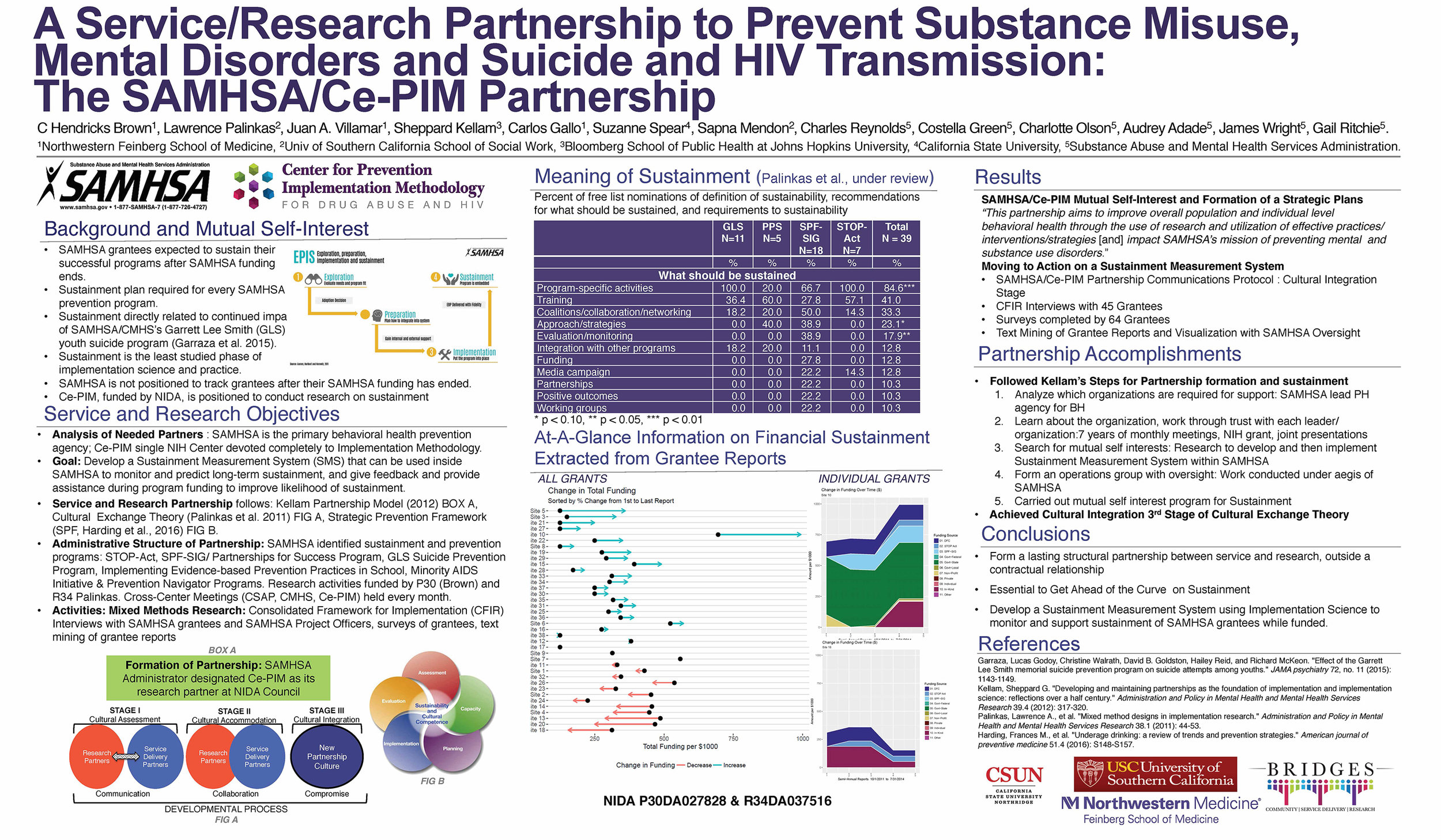
Results: This partnership is based on mutual self-interest, focusing as it does on SAMHSA’s unique leadership and responsibility to “yield better outcomes for people with, or at risk for, mental and substance use disorders,” and Ce-PIM’s focus on bringing methodologic rigor to both the research and practice of implementing effective prevention programs. Specifically, our common interest involved improved sustainment of SAMHSA’s prevention programs after funding cycles ended. Specific structures and processes were developed to sustain and strengthen this partnership. Internal changes were required for both SAMHSA and Ce-PIM to accommodate to this new partnership. We discuss these structures in the context of a collaborative effort to predict and improve sustainment of five prevention programs at SAMHSA; CSAP’s Strategic Prevention Framework State Incentive and Partnerships for Success, CSAP’s STOP Act as an extension of the Drug Free Communities, CMHS’ Garrett Lee Smith State-sponsored Youth Suicide Prevention Program, CMHS’ Implementing Evidence-Based Prevention Practices in Schools, and the Minority Serving Institutions Partnerships with Community Based Organizations. We discuss the development of a low-burden sustainment measurement system for SAMHSA programs. This system is useful for measuring change and includes a survey of grantees and automated presentation of sustainment data extracted from grantee reports through data mining.
Conclusions: This partnership provides a general model for federal service agencies and researchers to collaborate. We point to future directions of mutual interest including the uses of technology in implementing prevention programs, addressing the needs of health disparity populations, and integration of behavioral health in primary care.
